
DTX3 amplification found in a small proportion of breast cancer patients; linked with increased proliferation
The degree of cell proliferation is one of the most powerful prognostic features in breast cancer. Deltex E3 ubiquitin ligase 3 (DTX3), a member of the Deltex family, is located on 12q13.3 and is involved in neurogenesis and Notch signaling. DTX3 has been suggested as a potential driver gene of cell proliferation in luminal subtypes of breast cancer and has been associated with poor prognosis. However, studies of DTX3 in different cancers have found different results; in esophageal cancer, DTX3 was associated with reduced proliferation of tumor cells, and in colorectal cancer, DTX3 was proposed as an endogenous control gene for gene expression analyses. In this study, the authors’ aimed to further investigate and characterize the role of DTX3 in breast cancer, specifically looking for associations between DTX3 copy number and measures of cell proliferation.
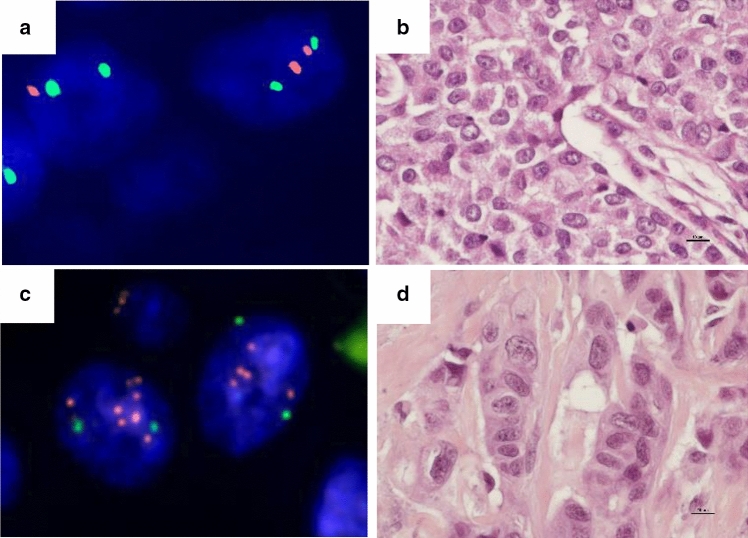
Fluorescent in situ hybridization (FISH) was used to assess DTX3 copy number in 542 breast cancer cases from a large historical cohort of women. Chromosome enumeration probe 12 (CEP12) was used to tag the chromosome 12 centromere as a control. For each case, DTX3 and CEP12 copy numbers were recorded in 20 non-overlapping tumor cell nuclei. Mean DTX3 and mean CEP12 copy number were estimated and cases were initially separated into three categories: mean copy number <4, mean ≥4<6, and mean ≥6. CEP12 copy number increase was infrequent, with only seven cases (1.3%) with a mean CEP12 ≥4<6 and one case (0.2%) with a mean CEP12 ≥6. Mean DTX3 copy number ≥4<6 was found in 20 cases (3.7%) and mean DTX3 copy number ≥6 was found in three cases (0.6%). Of the 23 cases with an increase in mean DTX3 copy number, only four cases had a concurrent increase in mean CEP12 copy number. This represented a statistically significant amplification of DTX3 in this small proportion of breast cancer cases (p < 0.0001).

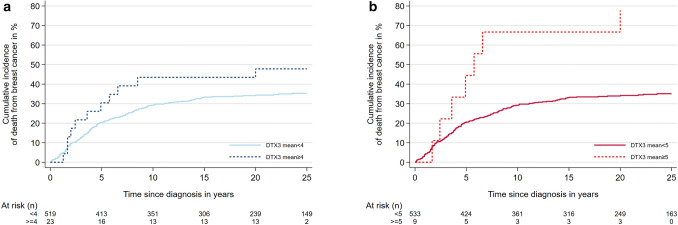
Due to the fact that only three cases had mean DTX3 copy number ≥6, the authors reclassified cases for further statistical analysis. Point estimates suggested that cases with DTX3 amplification had higher proliferation, higher histologic grade and a poorer prognosis than cases without DTX3 amplification, but the statistical significance of the association depended on the choice of cut-off. For example, with regards to proliferation, a statistically significant association between DTX3 amplification and Ki67 level was only found using the <4 / ≥4 cut-off (p=0.03) whereases a statistically significant association between DTX3 copy number and mitotic counts was found using both the <4 / ≥ 4 < 6 / ≥ 6 cutoff (p=0.03) and the <4 / ≥4 cut-off (p=0.009) but not the <5 / ≥5 cutoff (p=0.3). An association between DTX3 copy number and histological grade was found using both the <4 / ≥ 4 < 6 / ≥ 6 cutoff and the <4 / ≥4 cutoff (both p<0.001), with tumors with DTX3 amplification being of higher histological grade. Finally, death from breast cancer was higher among cases with mean DTX3 copy number ≥5 versus mean <5 (p=0.003); this statistical significance was not seen using the <4/ ≥4 cut-off (p=0.17).
Though DTX3 amplification occurred in only a small proportion of cases (less than 5%), in this era of personalized medicine, it may still prove to be of clinical relevance as a prognostic biomarker. Similar to earlier studies of breast cancer, this study reported a positive association between DTX3 copy number and measures of cell proliferation. It is possible that DTX3 may play different roles in different cancers, though much more research is needed. The authors also noted a trend in their sample between DTX3 copy number increase and age at diagnosis; in their cohort, mean age at diagnosis was lower among cases with DTX3 amplification compared to cases with DTX3 <4 (72.6 years vs. 75.4 years). The mean age at diagnosis was also much higher in their cohort (with DTX3 amplification <5%) than in similar studies that reported up to 18% of cases with DTX3 amplification (mean age 75 years vs. 58 years, respectively). Since the prognostic effect of proliferation is age-dependent, with a stronger prognostic influence among younger breast cancer patients, further research on DTX3 amplification in younger breast cancer patients could help to reveal the role of DTX3 copy number in breast cancer.
